小心类风湿关节炎治疗中的“伏地魔”!结核危(2)
ATTAIN研究 [16] :一项随访至5年的随机、3期试验表明,阿巴西普长期治疗期间无结核病例报道;
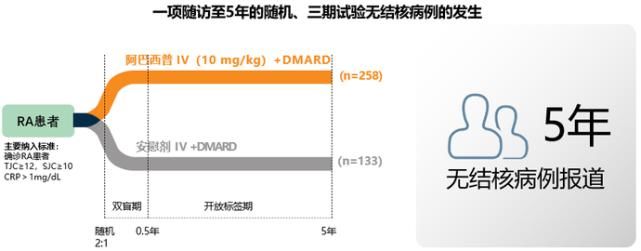 图2:ATTAIN研究中,随访至5年阿巴西普组无结核病例发生[16]
图2:ATTAIN研究中,随访至5年阿巴西普组无结核病例发生[16]
IM101-100研究 [17] :一项随访至7年的多中心、随机、2期试验表明,阿巴西普组无结核病例报道;
 图3:IM101-100研究中,随访至7年阿巴西普组无结核病例发生[17]
图3:IM101-100研究中,随访至7年阿巴西普组无结核病例发生[17]
基于以上结核易感性分析得出,阿巴西普的结核发生风险低,安全性相对较好。
3
RA患者使用生物制剂的结核管理
生物制剂的出现使RA治疗迈上了新征程,其在带来显著疗效的同时也存在着一定的安全风险,如结核感染风险。如何平衡其获益和风险,是我们在RA治疗中需要掌握的一门独特的“艺术”。
在RA治疗中,为降低患者结核感染风险,应强调临床管理规范:
不同生物制剂所带来的结核感染风险不一样。2018年亚太风湿病学会联盟(APLAR)更新的指南中指出,若患者具有结核病史或是潜伏性结核感染,应选择除TNF抑制剂以外的靶向治疗 [18] 。尽可能地选择结核风险较低的生物制剂(如阿巴西普)进行治疗;
在各大指南,如2015美国风湿病学会(ACR) [19] 及2018APLAR指南 [18] 中均指出,开始免疫调节治疗前,应该对患者进行结核菌暴露和感染的筛查,查看有无潜在结核感染;在治疗中,通过每年的结核病检测进行密切监测;
 图4:RA患者使用生物制剂前的结核筛选[20]
图4:RA患者使用生物制剂前的结核筛选[20]
结核筛查试验阳性的患者(或潜伏结核患者)应按照诊疗标准进行常规治疗后再开始生物制剂治疗。
4
小结
结核病在全世界流行广泛,我国更是其高发地区。RA患者中结核发病率较一般人群高,在其治疗中尤其需要注意潜在的感染风险。
不同生物制剂由于作用机制不同,所带来的结核感染风险也有所差异。在多项长期临床研究中,阿巴西普表现出良好的安全性,结核发生风险低,能一定程度避免生物制剂使用过程中的感染风险。
考虑使用生物制剂的RA患者应加强潜伏性结核感染的筛查,做好早期预防,密切监测,积极治疗。
参考文献:
[1] 高兆婷. 结核病的症状、危害与治疗[J]. 大科技, 2018, 3: 301.
[2] 中华人民共和国中央人民政府.世界防治结核病日:近5年来中国结核发病率年递降3.4%[EB/OL]. 张朝辉, 严晶晶. 我国结核病现状及防治措施[J].海南医学, 2018, 29 (23): 3386-3389.
[4] Carmona L, Hernández-García C, Vadillo C et al. EMECAR Study Group. Increased risk of tuberculosis in patients with rheumatoid arthritis[J]. J Rheumatol, 2003, 30:1436-1439.
[5] 杨峻, 何永玲, 唐文军, 等. 结核感染与机体免疫反应机制研究进展[J]. 右江医学, 2019,47(3): 223-226.
[6] Jick SS, Lieberman ES, Rahman MU, et al. Glucocorticoid use, other associated factors, and the risk of tuberculosis[J]. Arthritis Rheum, 2006, 55: 19–26.
[7] 吴杰炜,李升锦. 类风湿关节炎患者并发结核感染的研究进展[J]. 世界最新医学信息文摘, 2019, 19 (28): 54-64.
[8] Kammüller M, Tsai TF, Griffiths CE, et al. Inhibition of IL-17A by secukinumab shows no evidence of increased Mycobacterium tuberculosis infections[J]. Clin Transl Immunology, 2017 Aug 25, 6(8): e152.
[9] 吴汉霞, 张荣波, 杨剑. 细胞因子在结核病中的研究进展[J]. 华南国防医学杂志, 2010, 24 (4): 322-324.
[10] Mayer-Barber KD, Sher A. Cytokine and lipid mediator networks in tuberculosis[J]. Immunol Rev, 2015 Mar, 264(1):264-75.
[11] Gómez-Reino JJ, Carmona L, Valverde VR, et al. Treatment of rheumatoid arthritis with tumor necrosis factor inhibitors may predispose to significant increase in tuberculosis risk: a multicenter active-surveillance report[J]. Arthritis Rheum, 2003, 48(8):2122-2127.
[12] Westhovens R, Robles M, Ximenes AC, et al. Clinical efficacy and safety of abatacept in methotrexate-naive patients with early rheumatoid arthritis and poor prognostic factors[J]. Ann Rheum Dis,2009 Dec,68(12):1870-7.
[13] Bathon J, Robles M, Ximenes AC, et al. Sustained disease remission and inhibition of radiographic progression in methotrexate-naive patients with rheumatoid arthritis and poor prognostic factors treated with abatacept: 2-year outcomes[J]. Ann Rheum Dis, 2011 Nov, 70(11):1949-56.
[14] Weinblatt ME, Schiff M, Valente R, et al. Head-to-head comparison of subcutaneous abatacept versus adalimumab for rheumatoid arthritis: findings of a phase IIIb, multinational, prospective, randomized study[J]. Ar thritis Rheum, 2013 Jan, 65(1):28-38.
[15] Schiff M, Weinblatt ME, Valente R, et al. Head-to-head comparison of subcutaneous abatacept versus adalimumab for rheumatoid arthritis: two-year efficacy and safety findings from AMPLE trial[J]. Ann Rheum Dis, 2014 Jan, 73(1):86-94.
文章来源:《华南国防医学杂志》 网址: http://www.hngfyxzz.cn/zonghexinwen/2020/1110/351.html
上一篇:没有了
下一篇:投档分排名前100高校,深圳大学等17所四非高校,